Type 2 Diabetes Medication: Balancing Cost and Value
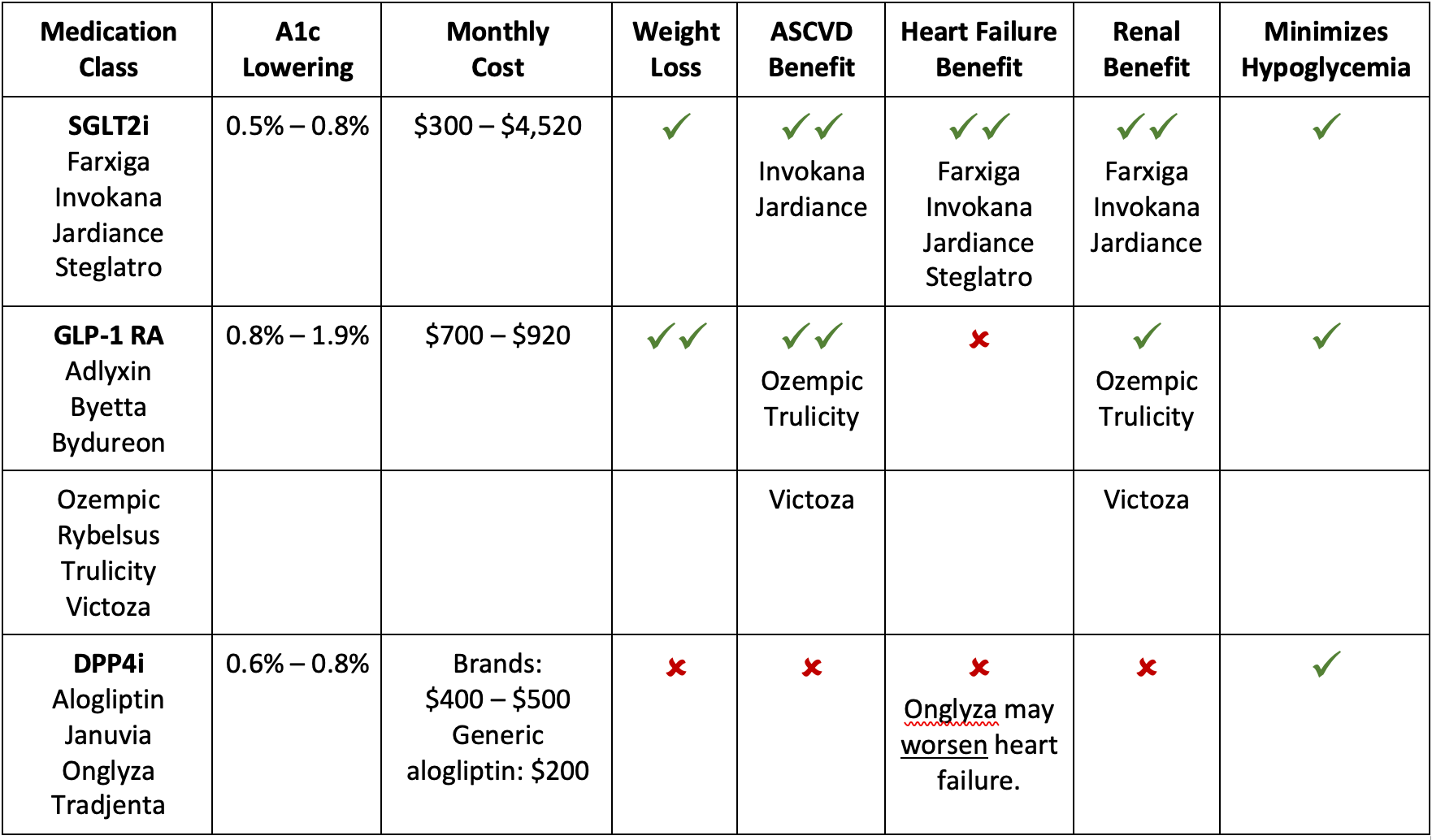
Appropriate medication therapy for type 2 diabetes is important for success in value-based care. A1c control, medication adherence and medication costs are metrics that many payers evaluate. However, managing these medications can be challenging, especially when insurance coverage and cost can vary significantly from patient to patient. After optimizing metformin, most patients will require a second-line agent for glycemic control. Dipeptidyl peptidase-4 inhibitors (DPP4i), glucagon-like peptide-1 receptor agonists (GLP-1 RA), and sodium-glucose co-transporter 2 inhibitors (SGLT2i) are commonly used after metformin. These medications are all high cost, so it is important to choose a medication that provides high value if using any of these classes. The table below can assist with selecting patient-specific, high-value medications to optimize value-for-dollar spending for both patients and payers.
Lower-Cost Options
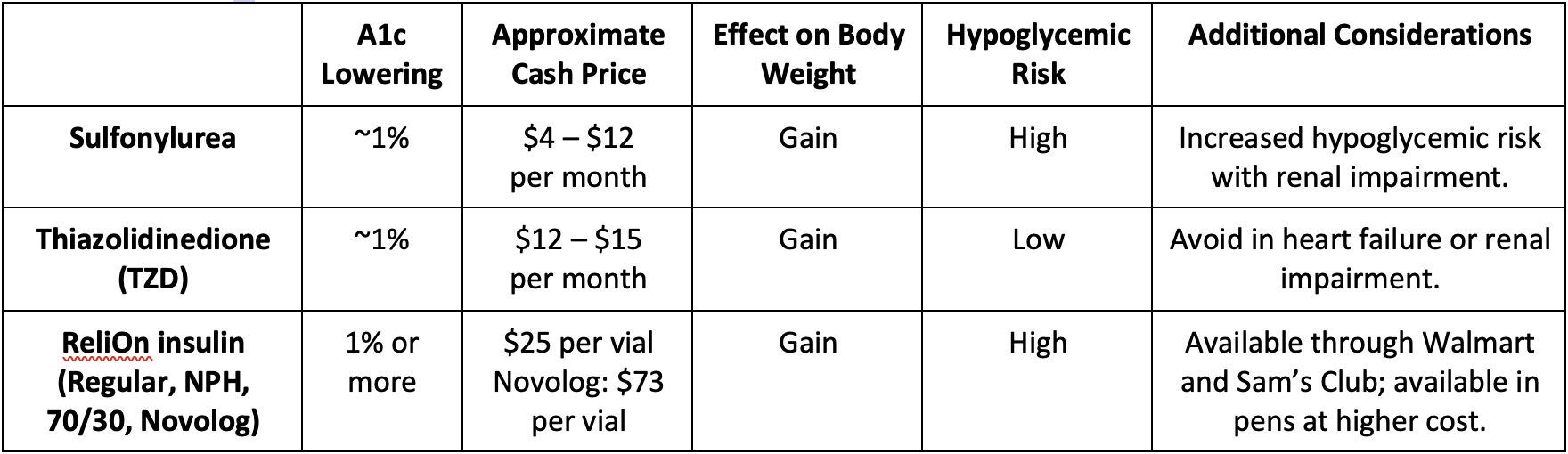
Some patients have significant affordability concerns that drive the selection of second-line agents and limit the use of DPP4i, GLP-1 RA or SGLT2i medications. The following table provides an overview of the most affordable second-line agents.
Another option is to consider a combination product. While these often have higher cash prices, for some patients with insurance it results in fewer copays and overall savings compared to single-agent preparations. Patients can contact their insurance company to see if a combination product is more cost-effective for their plan. There are numerous combination products available, and it can be difficult to determine what medication classes are included. The chart below provides an overview of which classes have combination products available.

Additional Resources
The American Diabetes Association 2022 Standards of Medical Care in Diabetes has a section devoted to medication therapy, which provides more detailed information. Consider bookmarking these pages to have a quick reference guide:
Table comparing medication classes on efficacy, weight effects, cardiovascular/renal benefits, cost and dosing information.
Flowchart for selecting medications based on patient-specific needs (cardiovascular/renal concerns, hypoglycemia risk, weight effects, cost).
Flowchart for adding and adjusting injectable therapies, specifically insulin and GLP-1 RA.
References:
American Diabetes Association Professional Practice Committee; 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2022. Diabetes Care 1 January 2022; 45 (Supplement_1): S125–S143. https://doi.org/10.2337/dc22-S009
Clinical Resource, Drugs for Type 2 Diabetes. Pharmacist’s Letter/Prescriber’s Letter. December 2020.
Clinical Resource, Comparison of Insulins. Pharmacist’s Letter/Prescriber’s Letter. September 2021. [370901]
Payer Feedback
Diabetes care quality measures play a significant role in all of our payer contracts, which is why four of the six metrics on our 2022 Single Scorecard involve the care of patients with diabetes. Success in these metrics will not only lead to better outcomes for our diabetic patients; it will also generate financial success in our value-based contracts.
So, how are we doing according to the payers? The Medicare Advantage data probably tells the story best: We have some work to do, most significantly in the area of diabetes, blood sugar controlled (A1c <8).
Diabetes Care Quality Measures
Medicare Advantage Programs: Star Ratings
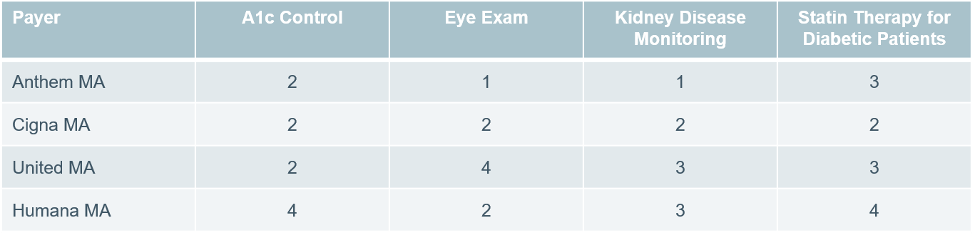
Across our Medicare Advantage programs, C3 performance is only at a 2-star rating for diabetes control. This is below the threshold needed to earn incentives in this metric. Since this is a triple-weighted measure in the MA space, this performance is heavily impacting our overall star ratings so we will continue to focus on this measure throughout the year.
Notes:
- Anthem MA and Humana MA reporting through October 2021; Cigna MA and United MA reporting through November 2021.
- Despite having 4 stars in A1c Control in Humana MA, we are not meeting the minimum target for the model practice quality incentive program.
- Payer-specific measures may not always be identical to Single Scorecard measures.font